
SHOULDER CONDITIONS
")
Shoulder Injuries
Frozen Shoulder
Frozen shoulder (adhesive capsulitis) is a painful condition characterised by progressive stiffness and loss of movement in the shoulder joint. It often develops gradually and can significantly impact daily activities such as dressing, reaching or sleeping comfortably. The condition typically progresses through stages and may take many months to resolve. While early management includes pain control, physiotherapy and targeted injections, some cases fail to improve with conservative treatment. In these situations, arthroscopic release or manipulation under anaesthesia can restore movement, reduce pain and accelerate recovery.
Frozen Shoulder
What is Frozen Shoulder?
Your shoulder is made up of three bones that form a ball-and-socket joint. They are your upper arm (humerus), shoulder blade (scapula), and collarbone (clavicle). There’s also tissue surrounding your shoulder joint that holds everything together. This is called the shoulder capsule.
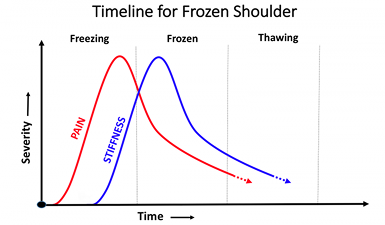
With frozen shoulder, the capsule becomes so thick and tight that it’s hard to move and any movement is painful. This tends to progress and gradually, gets worse. The pain and stiffness reach a climax point and then finally go away, the reduction in pain and stiffness is also a gradual process. This can take anywhere from a year to 3 years.
Causes
It’s not clear why some people develop it, but some groups are more at risk.
Frozen shoulder happens more often in women than men, and you’re more likely to get it if you’re between the ages of 40 and 60. Your risk might also go up if you’re in the process of recovering from a medical condition like a stroke, or surgery like a mastectomy that keeps you from moving your arm.
Certain medical conditions can increase your risk too. You may also be more likely to get frozen shoulder if you have diabetes. About 10% to 20% of people with diabetes get frozen shoulder. Other medical problems like heart disease, thyroid disease, or Parkinson’s disease are linked to frozen shoulder, too.
Stage One
The patient usually gradually develops initially pain following restricted range of motion (stiffness) of the shoulder joint. Typically there is no particular cause though a frozen shoulder may be triggered by a simple trauma i.e. following a fall or other injury or sometimes after surgery either on the shoulder or other operations eg. Removal of gallbladder or cardiac surgery. The first stage of frozen shoulder is the most painful and patients typically have pain if they suddenly move the shoulder (jerk pain) and pain at night that may disturb sleep. Patients may have difficulty with activities of daily living such as dressing , washing and household chores. Stage one generally takes in the order of 4-6 months though there can be quite a variation.
Stage Two
In the second stage the shoulder is less painful though remains restricted and the patient will have difficulty performing many activities particularly moving the arm behind the back for example to secure a bra.
Stage Three
In stage the pain has resolved completely and the range of motion returns to normal. The total time for the range of motion to return completely ranges from 18 months to 2 year and in fact may be longer in patients with diabetes or hypothyroidism.
Investigations
Frozen shoulder can usually be by diagnosed on the basis of the patient’s history and examination. There are few other conditions in the shoulder which lead to such rapid loss of range of motion and restriction. A plain X Ray is useful to exclude arthritis of the shoulder or if there is a history of trauma any dislocation or fracture. An MRI scan can help exclude other conditions such as a rotator cuff tear. An MRI scan will not however definitively diagnose a frozen shoulder and in fact in this age group there are often unrelated coincidental findings such as degenerative tears of the labrum, degenerative changes of the acromioclavicular joint and partial tears of the rotator cuff which are normal findings in patients over the age of 40.
Frozen Shoulder
Treatment
Frozen shoulder is a generally very painful in the initial stages and it is important to take adequate painkillers and rest the shoulder if it very painful. There is no advantage in trying to vigorously mobilising the shoulder at this stage as it is too inflamed and will only aggravate the pain.
In the first stage of the condition a corticosteroid injection can be very helpful in improving pain. Gentle stretching to maintain motion is useful but avoid painful movements. This can be repeated a second time as needed.
Hydro-dilatation is a radiological procedure which can be used in Stage 1 or 2 frozen shoulder. Local anaesthetic and steroid are injected into the shoulder Joint under image control. This is performed as an outpatient under local anesthetic.
In the majority of patients surgical intervention is not required. However, it is important to remember that if you suffer from a frozen shoulder on one side, you may also develop frozen shoulder on the other.
Approximately 10% of patience with frozen shoulder who do not respond two injections or Hydrodilatation may require surgical intervention.
Arthroscopic Capsular Release
This is keyhole surgery to release the contracted capsule (link to arthroscopic release) .
The aim of the surgery is to release the contracted capsule using an instrument called a radiofrequency probe. The usual findings at the time of surgery is that the capsule is often red and inflamed and much thicker than it should be.
Unfortunately, patients who have diabetes or hypothyroidism tend to get a more severe form of frozen shoulder and often they require surgical intervention. The good news is that once a frozen shoulder resolves it never recurs.
Frozen Shoulder
")
")