
SHOULDER CONDITIONS
Shoulder Injuries
Rotator Cuff Injuries
Rotator cuff injuries are common, particularly in overhead and contact sports such as GAA football, hurling and rugby. They range from tendon inflammation and partial tears to full-thickness rotator cuff tears. The rotator cuff is a group of muscles and tendons that stabilise the shoulder joint while allowing controlled movement and strength. Injury to these tendons can result in pain, weakness, night discomfort and reduced function, particularly with lifting or overhead activity. While some minor injuries respond well to physiotherapy and rehabilitation, more significant tears do not heal on their own and may progress over time. Surgical repair, most commonly performed arthroscopically (key-hole surgery), can restore tendon attachment, improve strength and function, and help patients return safely to work, sport and daily activity.
Rotator Cuff Injuries
How did I injure my Rotator Cuff?
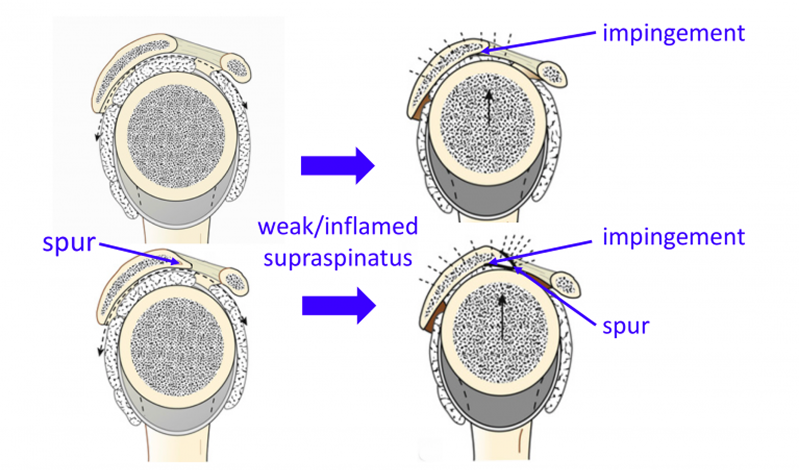
When the supraspinatus tendon becomes inflamed it is weakened and allows the humeral head to “ride up” on the undersurface of the coracoacromial arch leading to impingement This is compounded in the presence of a subacromial spur
The Supraspinatus Tendon lies over the top of the Humeral Head (Ball) and runs underneath the Acromion (arch of the Scapula).
The action of the Supraspinatus Tendon is to help Elevate and ABduct the arm, it is one of the most heavily used Rotator Cuff tendons and the one that is most prone to wear and tear changes.
The clearance space for the healthy Supraspinatus Tendon to run underneath the front of the Acromion is usually adequate. However, there is usually not a great amount of reserve space available. As a result, if the Tendon becomes at all inflamed or enlarges, for any reason, it can begin to ‘impinge’ or rub on the undersurface of the Acromion. Supraspinatus Tendonitis and Impingement are inter-changeable names to describe inflammation and swelling of the Supraspinatus Tendon, which usually has a ‘wear and tear’ element.
When the Tendon becomes inflamed it is also weakened which makes it is less effective at pulling the head downwards. These factors can then lead to further damage or inflammation to the Tendon, starting a ‘vicious circle’ of ‘Impingement’.
The shape and angle of inclination of the Acromion can vary between people. Sometimes people refer to a ‘hook’ or ‘spur’ at the front of the Acromion that is related to their Impingement. As a general rule, the shape of someone’s Acromion does not change significantly over time, and it is likely that their Acromion has always been that shape resulting in them having less ‘reserve’ space available for any underlying tendon enlargement.
Acromioclavicular (AC) joint osteoarthritis often develops in patients as they get older. Sometimes an inferior osteophyte from the AC joint can also impinge on the rotator cuff.
There is a small Bursa (fluid filled sac) that lies on top of the Supraspinatus Tendon and beneath the Acromion. Its job is to try and ease the movement of the tendon underneath the bone. This can sometimes get inflamed, along with the tendon, but often has eroded away over time.
Whilst the mechanism of Impingement is a major factor in the development of Supraspinatus Tendonitis, there are a number of other extrinsic and intrinsic factors that can also play a part.
What are the symptoms of a Supraspinatus Tendonitis/Impingement
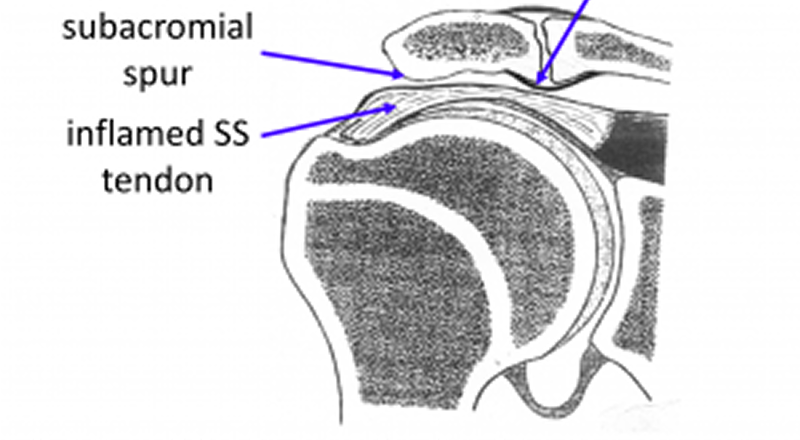
diagram of the front of the shoulder demonstrating an inflamed supraspinatus tendon “impinging” on a subacromial spur and AC joint osteophyte
As ‘wear-and-tear’ plays a considerable part in the development of Supraspinatus Tendonitis the onset of symptoms can often be quite insidious. As a result, many people find that their Supraspinatus Tendonitis gradually develops over time. In other cases, a specific injury or incident can aggravate the degenerate tendon and spark off a sudden onset of symptoms.
The early symptoms of Supraspinatus Tendonitis tend to be a background pain over the shoulder with particular discomfort when elevating the shoulder within the ‘Painful Arc’. The shoulder is often uncomfortable to lie on at night. As symptoms deteriorate the shoulder becomes increasingly painful more of the time. Pain tends to occur on more directions of movement and the shoulder can appear to become weaker. Night discomfort often becomes more of a feature. With chronic shoulder pain, the muscles that help to stabilize the scapula often try to hold the shoulder up, in a more protected position. Overtime these muscles can begin to ache so that the pain can appear to radiate up towards the neck and over the shoulder blade.
How do you Diagnose Supraspinatus Tendonitis (Impingement)?
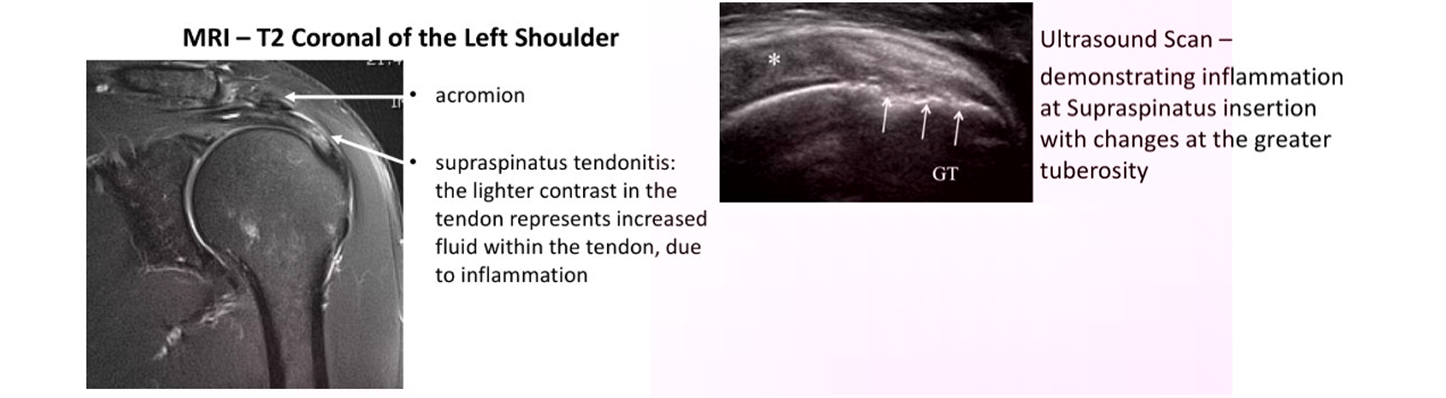
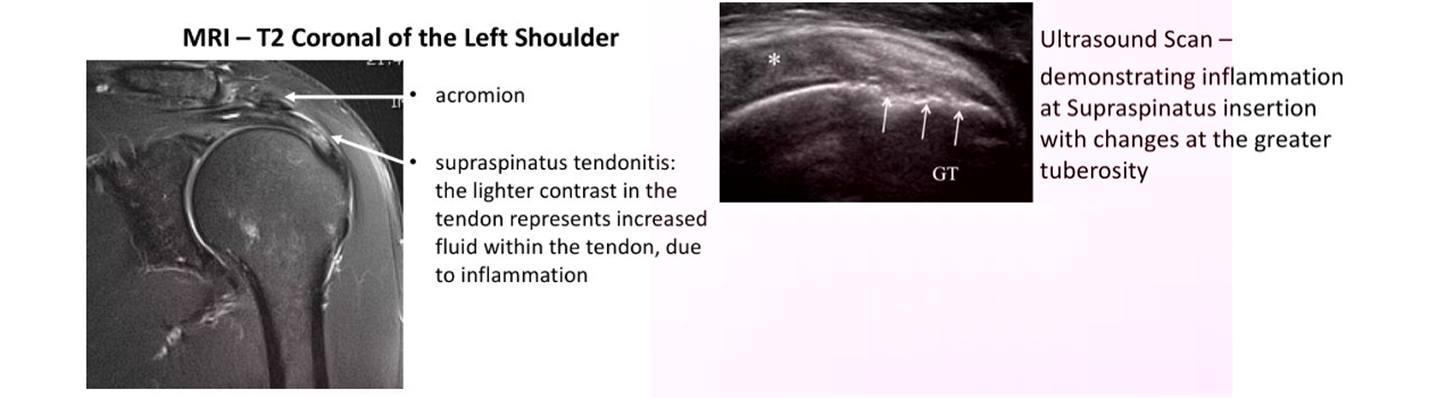
MRI – T2 Coronal of the Left Shoulder
- History – Most people notice a gradual onset of pain and discomfort over the top and side of their shoulder. Sometimes people can identify a specific injury or incident that triggered their problem. They may notice particular pain on elevating their arm and in bed at night. As the condition deteriorates they may get pain more of the time and on more directions of movement. They also might notice some weakness.
- Examination – Occasionally the patient can experience some discomfort on palpation over the front edge of their Acromion. People may have a ‘painful arc’ on elevating their shoulder and positive ‘impingement signs’. People with Supraspinatus tendonitis often have associated problems with Acromioclavicular Joint (ACjt) arthritis and Long Head of Biceps Tendonitis and may have symptoms and signs of these as well.
- Investigations –
- X-Ray – An x-ray does not usually demonstrate the soft-tissues of the Rotator Cuff. However, the shape of the acromion, ACjt osteoarthritis and calcific deposits can sometimes be noted.
- Ultrasound Scan (USS) – An USS will nicely demonstrate the Rotator Cuff tendons and the Long Head of Biceps. It is able to show whether there is a tendonitis, partial or full thickness tear of the tendons.
- MRI Scan– An MRI scan is the best investigation to visualize the rotator cuff. It can show all of the tendons and whether there is a tendonitis, partial or full thickness tear. It will also demonstrate the acromion and ACjt and their relationship with the tendons. An MRI scan will also show up any other problems around the shoulder.
What is the Rotator Cuff?
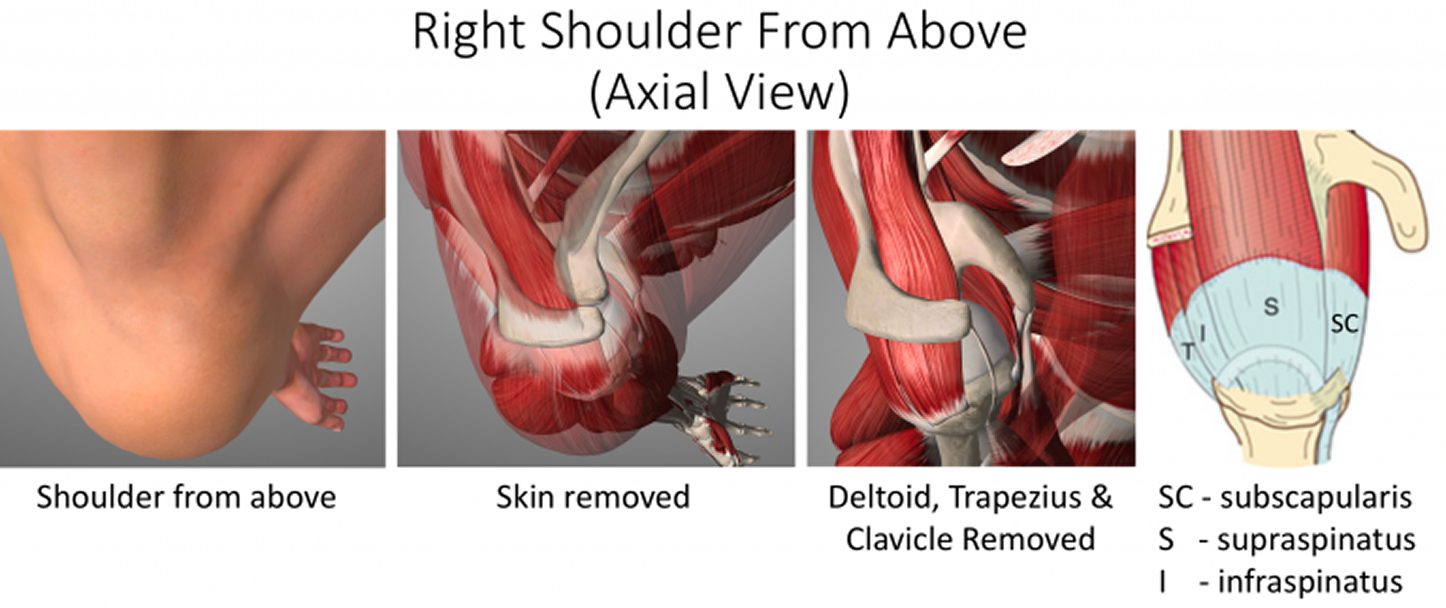
This refers to a group of tendons that join the muscles that move and support the shoulder to the bone of the upper arm. The tendon is most vulnerable to damage where it is attached to the humerus bone and runs underneath the upper part of the shoulder blade- acromion. Rotator cuff tears are the most common problem in the shoulder and commonly cause pain and restricted range of motion.
Rotator Cuff Tears (Torn Tendon)
- Everyone’s Rotator Cuff Tendons undergo ‘wear-and-tear’ over time. This can lead initially to a Tendonitis, which is an inflammation and fraying of the tendon. Then as the tendons become weakened, it thins out, and can lead to Partial or Complete tears.
- This process is often going on quietly in the background and many people, over time, develop tears without any symptoms and without knowing about it. In an MRI scan study of people over 60 who felt that they had no problems with their shoulder, over 40% had a tear of some size of their Rotator Cuff on their scans!
- However, some people with a Rotator Cuff Tears do develop symptoms. These maybe sparked off by a specific incident or accident, where an acute tear occurs in an already weakened or previously torn tendon. In other people the symptoms may develop slowly representing the progression of a Supraspinatus Tendonitis.
- Regardless of the way that the symptoms of a Rotator Cuff Tear start, when they do occur, they usually require some form of treatment to settle it down.
Can the Rotator Cuff heal on its own?
The short answer to this is NO
- When the tendon is torn the pull of the muscle will retract the torn edge away from its bone attachment
- The only way the tendon can heal is if it is re-attached
- However not every torn tendon will lead to symptoms and many patients maintain or can regain full shoulder function without requiring a repair
Types of Rotator Cuff Tears
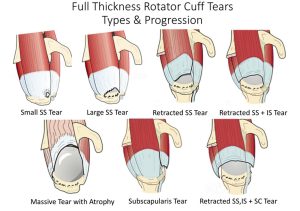
There are many different types of Rotator Cuff Tears and different ways that they can be classified. I prefer to look at Tears in the way that they can be treated. Mr Mullett likes to think of them as either being Acute or Chronic, which Tendons have been Torn, whether they are Partial or Full Thickness Tears, how big they are and whether it will be technically possible to repair them. Other considerations are the quality of the tissue and fatty atrophy, other associated shoulder problems and the age, health and expectations of the individual patient.
- Acute v Chronic Tears – most Rotator Cuff tears are chronic and have slowly developed over time. However, sometimes patients can sustain an acute or an acute-on-chronic tear following a specific injury or event. If in Acute Tear is repaired within 3 – 4 months of its onset, it is likely that it will heal better than if the repaired later. For chronic tears this time window is less important.
- Partial v Full Thickness Tears – Partial Thickness Tears tend to occur in younger patients and at an earlier stage of Rotator Cuff Disease.
- 80% occur on the articular side of the tendon, which is thought to be the result of a ‘watershed’ in the blood supply to the tendon
- Not all Partial Thickness Tears need to be repaired as they can sometimes heal or may not progress.
- However, as a general rule, the bigger the size of the tear, the younger the age of the patient and the more severe the symptoms are indications to surgically repair the Tendon as the tear is likely to progress over time.
- Full Thickness tears generally will NOT heal and probably, over time, will propagate/spread further. Most symptomatic Full Thickness Tears will usually require a repair to settle the symptoms.
- Size of the Tear – Rotator cuff tears tend to propagate over time.
- Tear size tends to be measured with regards to the distance with which the torn tendon has retracted from its insertion on the greater tuberosity.
- With advances in surgical technique and equipment it is now possible to repair even very large tears. However, there are still some situations where the tear is so massive, the tendon has begun to disappear or is so stuck and retracted that it may not be technically possible to undertake a repair.
Other considerations with regards to Rotator Cuff Tears
Which Tendon is Torn? – Although the Supraspinatus Tendon is the most commonly torn tendon, Infraspinatus and Subscapularis tears can also occur. Sometimes more than one tendon may be torn at the same time. The best way to treat specific tendons and combination tears can differ depending on the tendons involved.
Quality of the Torn Tendon – Rotator Cuff Tears usually occur in degenerate tendons. Sometimes the degeneration / ‘wear-and -ear’ is so advanced that the actual quality of the torn Tendon is not mechanically strong enough to hold a repair and probably will not heal.
Fatty Atrophy – When a Tendon is torn, the muscle that it was connecting to the bone will no longer be able to work and undergoes Disuse Atrophy. If this situation is sustained the muscle cells may then begin to be replaced by fat cells, Fatty Atrophy. Unfortunately, this is an irreversible process and, even if the Tendon is repaired and the muscle re-activated, the muscle cells cannot be restored. If the muscle of a torn tendon has undergone significant Fatty Atrophy, even if the tendon can be technically repaired, it will not regain its function.
Associated Shoulder Problems – Rotator Cuff Tears are often associated with other wear and tear problems in the shoulder. These include Long Head of Biceps Tendonitis, AC Joint problems and Shoulder Joint Osteoarthritis. How significant the Rotator Cuff Tear’s contribution is to a patient’s symptoms, when any of these associated problems are present, may determine how it is best treated.
Age, Health and Patient’s Expectations – Mr Mullett tends to look at age physiologically rather than Chronologically!! That said, younger patients usually have a better healing potential, are more active and will have higher functional expectations. As a result, they are likely to heal better and more quickly following a bigger procedure and may be more tolerant of undergoing a protracted recovery period to gain the best function possible. Older patients and patients with other significant health issues may not heal as well and are only looking for pain relief and a recovery of normal day to day function. They may be less prepared to undergo a ‘heroic’ procedure with a protracted recovery to gain the best function and would prefer a less complex procedure with a quicker recovery of acceptable function.
What are the Symptoms of a Rotator Cuff Tear?
As with a Supraspinatus Tendonitis, ‘wear-and-tear’ plays a considerable part in the development of Rotator Cuff Tears and the onset of symptoms can often be quite insidious. As a result, many people find that their symptoms gradually develop over time. In other cases, a specific injury or incident can create a tear or propagate further a chronic tear and spark off a sudden onset of symptoms.
There is a bulge on the side of the Humeral Head (Greater Tuberosity) where the Supraspinatus and Infraspinatus Tendons insert into the bone. As the shoulder moves, this bulge lies directly under the acromion between 60 and 120 degrees of elevation. This is the point where the space between the top of the Humeral Head and the Acromion is the narrowest. This is known as the ‘Painful Arc’ of movement.
The early symptoms of a Rotator Cuff Tear tend to be a background pain over the shoulder with particular discomfort when elevating the shoulder within the ‘Painful Arc’ and associated weakness. The shoulder is often uncomfortable to lie on at night.
As symptoms deteriorate the shoulder becomes increasingly painful all of the time. Pain tends to occur on more directions of movement and the shoulder can appear to become weaker. Night discomfort often becomes more of a feature.
With chronic shoulder pain, the muscles that help to stabilize the scapula often try to hold the shoulder up, in a more protected position. Overtime these muscles can begin to ache so that the pain can appear to radiate up towards the neck and over the shoulder blade.
How do you diagnose a Rotator Cuff Tear?
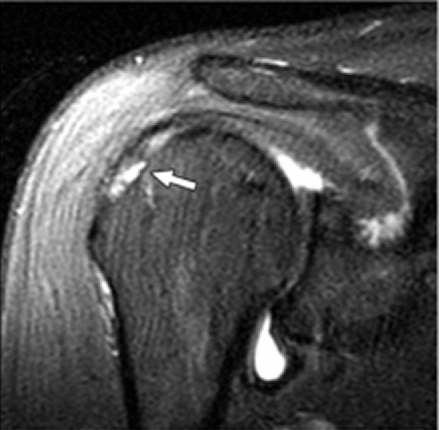
MRI Scan demonstrating an articular sided partial thickness tear of supraspinatus (T2 Sagittal View)
- History – Most people notice a gradual onset of pain and discomfort over the top and side of their shoulder. Sometimes people can identify a specific injury or incident that triggered their problem. They may notice particular pain on elevating their arm and in bed at night. As the condition deteriorates, they may get pain more of the time and on more directions of movement. They also might notice some weakness. In extreme cases they may not be able to actively elevate their shoulder at all.
- Examination – Occasionally the patient can experience some discomfort on palpation over the front edge of their Acromion. In the case of longstanding tears the Rotator Cuff muscles may undergo atrophy, which can be seen as ‘wasting’ of the muscles over the shoulder blade (scapula). People may have a ‘painful arc’ on elevating their shoulder and positive ‘impingement signs’. People with Rotator Cuff Disease often have associated problems with Acromioclavicular Joint (ACjt) arthritis and Long Head of Biceps Tendonitis and may have symptoms and signs of these as well.
- Investigations –
- X-Ray – An x-ray does not usually demonstrate the soft-tissues of the Rotator Cuff. However, the shape of the acromion, ACjt osteoarthritis and calcific deposits can sometimes be noted. In extreme cases of longstanding Rotator Cuff Tears the humeral head can be seen to have migrated superiorly under the acromion and even to have developed arthritis (Rotator Cuff Arthropathy)
- Ultrasound Scan (USS) – An USS will nicely demonstrate the Rotator Cuff tendons and the Long Head of Biceps. It is able to show whether there is a tendonitis, partial or full thickness tear of the tendons.
- MRI Scan An MRI scan is the best investigation to visualize the rotator cuff. It can show all of the tendons and whether there is a tendonitis, partial or full thickness tear. It will also demonstrate the acromion and ACjt and their relationship with the tendons. If there has been a longstanding tear the MRI can show evidence of how far the torn tendon has retracted and if there is any evidence of muscle belly atrophy. An MRI scan will also show up any other problems around the shoulder.
Rotator Cuff Injuries
Management of Rotator Cuff tendinitis

Many patients with a Supraspinatus Tendonitis can be successfully treated non-operatively with a combination of NSAIDs (Non-Steroidal Anti-Inflammatory Drugs) , Physiotherapy and use of steroid injections .
- Physiotherapy – Physiotherapy and specific Rotator Cuff Strengthening exercises are the main-stay of the initial treatment for Supraspinatus Tendonitis. By specifically strengthening the Supraspinatus muscle it can work and contract more efficiently pulling the humeral head downwards and allowing the tendon to move more freely. Anti-inflammatory medication can help pain and swelling
Subacromial Cortisone Injection –
- If patients have had painful impingment for greater then 4-6 weeks a subacromial steroid injection may be helpful. When injected into the Subacromial space it has the potential of settling severe inflammation, allowing the patient to undertake their rehabilitation exercises.
- A Subacromial Cortisone can be easily administered in the Out-Patient Clinic. It is a quick and relatively painless procedure. Afterwards patients can continue with their normal day-to-day activities. Occasionally patients can feel a bit of soreness around their shoulder later that day, but this usually passes fairly quickly.
- It often takes several days before someone notices the benefits following a Cortisone injection and sometimes several weeks. The Cortisone works in the background and there is no specific requirement to particularly rest the shoulder or to do extra exercises. The full benefits of a Cortisone injection are usually felt within a month. In some cases, the Cortisone may not give any benefit, this may be an indication of the severity of the Supraspinatus Tendonitis.
- A Cortisone injection only lasts in the body for a few days. Any benefit that someone gets from the Cortisone will be from its acute anti-inflammatory effect allowing the Supraspinatus Tendonitis to settle. If the symptoms do return after a while, it is not because the Cortisone has worn off, but because the inflammation has returned.
- Infections can occur after any type of injection but are extremely rare (1 in 15,000). If someone feels that they are developing an infection within 48 hours of a Cortisone injection they should seek advice from their Family Practitioner.
- Surgery for Supraspinatus Tendonitis – In some instances a Supraspinatus Tendonitis fails to respond, or continues to recur, despite adequate Physiotherapy and Cortisone treatment. In this situation the only treatment that is likely to settle the symptoms is Surgery.
Arthroscopic Subacromial Decompression
The best operation for someone with a Supraspinatus Tendonitis, that is refractory to treatment, is an Arthroscopic Subacromial Decompression. At the time of the surgery Mr. Mullett will examine the entire joint and then remove bone spurs and inflamed bursa thet are causing pain.
1. An Arthroscopic Subacromial Decompression can usually be done as a Day Case procedure and the patient’s shoulder does not need to be immobilized for anytime afterwards. The surgery aims to remove the part of the Acromion that has been causing the Impingement. It does not specifically deal with the underlying tendonitis. However, by enabling the Supraspinatus Tendon to run freely it allows for the Tendonitis to settle down. As a result it usually takes between 3 – 6 months to gain the full benefits of the procedure. It has a high success rate with around 95% of patients being happy with the result 6 months after their operation. (see ASD leaflet)
What are the symptoms of a Supraspinatus Tendonitis/Impingement
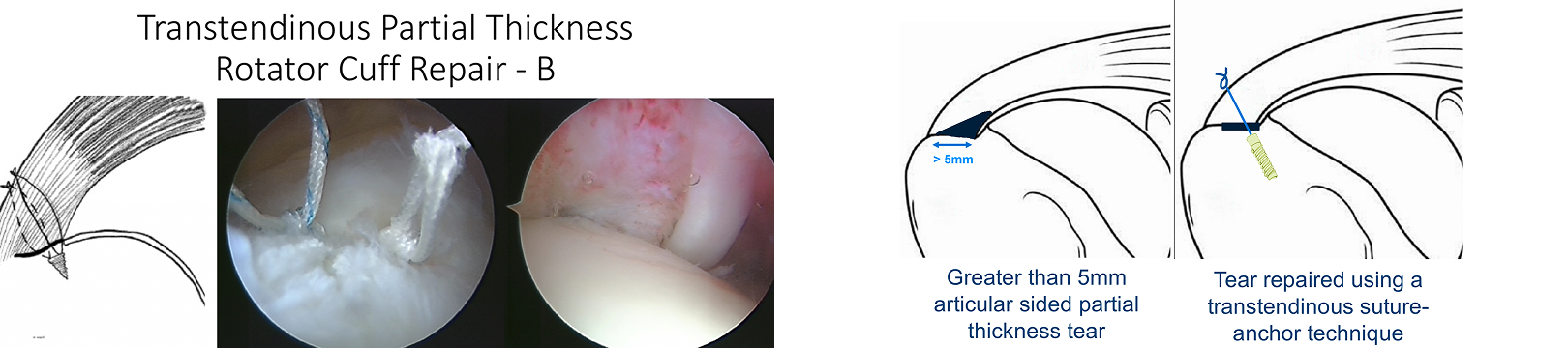
The sutures have been tied on the bursal side of the tendon, fixing the partial thickness tear securely down onto the bone
Management of Rotator Cuff Tears
- There is a vast variation between the specific symptoms, types and chronicity of a tear and the needs and expectations of patients who present with a symptomatic Rotator Cuff Tear
- There are also many different ways of treating and repairing Rotator Cuff Tears
- My approach to treating a patient with a symptomatic Rotator Cuff Tear is to assess the specific issues and nature of their problem and to then base my recommendation of how to treat their Rotator Cuff Tear, based on this
Surgery for Rotator Cuff Tears
- I undertake all of my Rotator Cuff Repairs using Arthroscopic Surgery (keyhole surgery)
- The basic aim of any Rotator Cuff Repair is to mobilise and freshen up the ends of the torn tendon, to freshen up the boney insertion on the humerus and then to position and re-attach the tendon back down to its original insertion, achieving a tensionless repair
- To achieve this there are multiple techniques, implants and strategies that can be used
- The descriptions of the procedures outlined below are based on the general technique. The specific details and pros and cons of the various implants and equipment that I use are covered in the Arthroscopic Surgery Section
find out more about Arthroscopic Shoulder Surgery….(Patient Information – Arthroscopic Shoulder Surgery)
How do you Diagnose Supraspinatus Tendonitis (Impingement)?
MRI – T2 Coronal of the Left Shoulder
- History – Most people notice a gradual onset of pain and discomfort over the top and side of their shoulder. Sometimes people can identify a specific injury or incident that triggered their problem. They may notice particular pain on elevating their arm and in bed at night. As the condition deteriorates they may get pain more of the time and on more directions of movement. They also might notice some weakness.
- Examination – Occasionally the patient can experience some discomfort on palpation over the front edge of their Acromion. People may have a ‘painful arc’ on elevating their shoulder and positive ‘impingement signs’. People with Supraspinatus tendonitis often have associated problems with Acromioclavicular Joint (ACjt) arthritis and Long Head of Biceps Tendonitis and may have symptoms and signs of these as well.
- Investigations –
- X-Ray – An x-ray does not usually demonstrate the soft-tissues of the Rotator Cuff. However, the shape of the acromion, ACjt osteoarthritis and calcific deposits can sometimes be noted.
- Ultrasound Scan (USS) – An USS will nicely demonstrate the Rotator Cuff tendons and the Long Head of Biceps. It is able to show whether there is a tendonitis, partial or full thickness tear of the tendons.
- MRI Scan- An MRI scan is the best investigation to visualize the rotator cuff. It can show all of the tendons and whether there is a tendonitis, partial or full thickness tear. It will also demonstrate the acromion and ACjt and their relationship with the tendons. An MRI scan will also show up any other problems around the shoulder.
- Rotator Cuff Tears usually occur in tendons that have undergone ‘wear and tear’ and, as the tear occurs, the degenerate tendon is no longer strong enough to withstand the mechanical forces placed on it
- When a Rotator Cuff Tendon is repaired it is still degenerate and, as a result, its healing potential is not as good as a normal, healthy tendon
- Surgical techniques and implant technology are constantly advancing and we are currently able to mobilise and successfully repair nearly all tendon tears
- However, despite this, a number of repairs still fail to heal
- This is likely to be due to the poor healing potential of degenerate tendons
The latest advance in Rotator Cuff Repairs, ‘Ortho-Biologics’, involves trying to improve and optimize the healing potential of degenerate tendons find out more about ‘Ortho-Biologics’….(Patient Information – Arthroscopic Surgery – Orthobiologics)
Factors that May Affect Rotator Cuff Healing
There are a number of factors that have a relative effect on a rotator cuff repair healing and include,
- Age of the patient
- Size of the tear and retraction
- Muscle atrophy
- Chronicity of the tear
- Smoking
Rotator Cuff Injuries
")
")
Rotator Cuff Injuries