
SHOULDER CONDITIONS
Shoulder Injuries
Shoulder Sport Injuries
Shoulder injuries are common particularly in collision sports such as GAA football, hurling and rugby. Common sporting injuries of the shoulder include shoulder dislocations, AC joint injuries, Rotator cuff Tears, Biceps Injuries and labral tears. The shoulder (ball & socket joint) is very mobile allowing great range of motion but because of this can either partially dislocate (subluxation) or fully dislocate. The damaged structures don’t tend to repair and this leads to a high rate of repeated subluxations or dislocations. Surgical reconstruction eith through arthroscopic (key-hole) or Open surgery can significantly reduce the likelihood of further instability.
Shoulder Injuries
How did I dislocate my shoulder?
Dislocations of the shoulder are one of the most common injuries to the shoulder, especially in younger athletes and those who participate in contact sports.
The shoulder joint is the most frequently dislocated joint of the body. Certain individuals are inherently “loose” or lax in their shoulders, which may place them at greater risk of instability.
The shoulder joint (gleno-humeral joint) is structured as a “ball-in-socket” joint. This allows for extreme ranges of motion. However due to the high mobility of the human shoulder joint and the fact that the socket is shallow there is a risk of shoulder dislocating ( shoulder instability). *for more information see anatomy dropdown above.
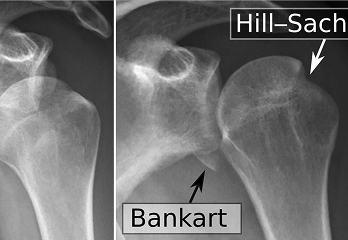
Since the socket is shallow, the shoulder relies on the soft tissue around the shoulder for stability. The labrum, a thickened cartilage layer around the glenoid, ligaments and capsule, provide most of the stability to the shoulder. The muscles of the rotator cuff and scapula also provide stability. Because it moves in several directions, your shoulder can dislocate forward, backward or downward, completely or partially, though most dislocations occur through the front of the shoulder ( anterior dislocation ) . In addition, ligaments that maintain the ball (humeral head) in the socket (glenoid) can be torn or stretched, often complicating the dislocation and make further dislocations more likely.
“Diagram shows action of of engaging Hill-Sachs”
The shoulder is most commonly dislocated when the arm is abducted and externally rotated, in a position as if you were throwing a ball. When there is a strong force with the arm in this position, the humeral head can dislocate out the front of the glenoid. When this occurs, it can either come partially out, which is termed a shoulder subluxation, or come entirely out, which is termed a shoulder dislocation. Although some people are able to reduce their shoulder themselves (put it back into joint), many others need to have their shoulder reduced in an emergency department mostly due to excessive surrounding muscle spasm. Patients who play contact sports such as GAA football or hurling or rugby are at higher risk of shoulder instability due to the collision nature of these sports. Male players are at a higher risk of shoulder instability. Some athletes have extra mobility of their joints (hyperlaxity) . This generally is a good thing as it can confer an athletic advantage but comes at an increased risk of joint dislocations including the shoulder joint.
What Symptoms does Instability Cause?
The shoulder is most commonly dislocated when the arm is abducted and externally rotated, in a position as if you were throwing a ball. When there is a strong force with the arm in this position, the humeral head can dislocate out the front of the glenoid. When this occurs, it can either come partially out, which is termed a shoulder subluxation, or come entirely out, which is termed a shoulder dislocation. Although some people are able to reduce their shoulder themselves (put it back into joint), many others need to have their shoulder reduced in an emergency department mostly due to excessive surrounding muscle spasm. Patients who play contact sports such as GAA football or hurling or rugby are at higher risk of shoulder instability due to the collision nature of these sports. Male players are at a higher risk of shoulder instability. Some athletes have extra mobility of their joints (hyperlaxity) . This generally is a good thing as it can confer an athletic advantage but comes at an increased risk of joint dislocations including the shoulder joint.

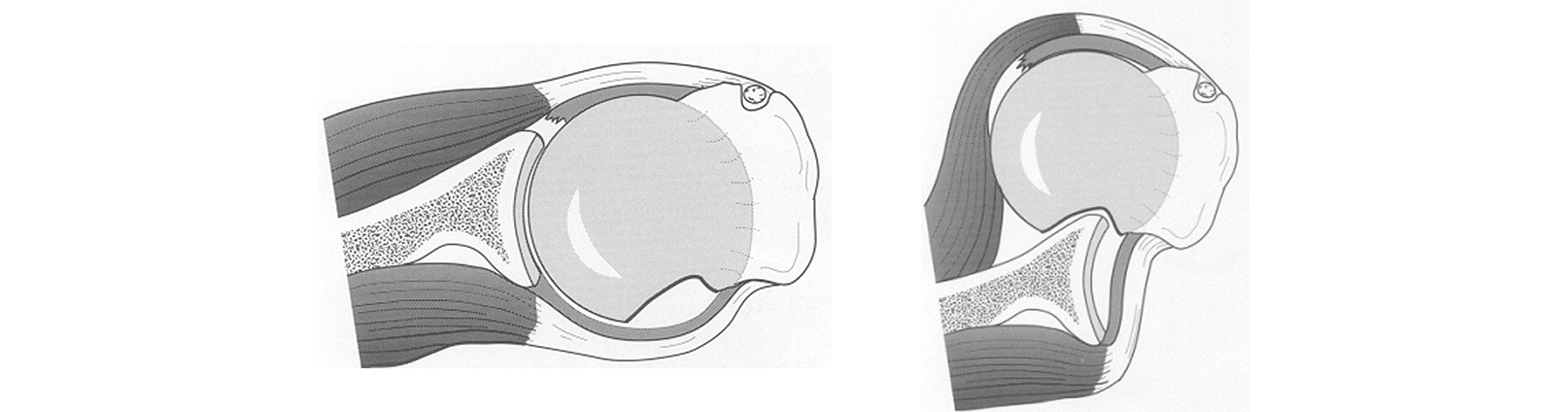
“Diagram shows labreal tear”
In the most severe example, the glenohumeral joint dislocates, meaning the ball completely separates from the socket. The ball needs to be relocated into the joint either on the pitch by a physio or doctor or if this is not available or it is not possible the player will need to attend the hospital to have it put back in (reduced) under sedation or occasionally under a full anaesthetic. After a first dislocation it is advisable to have an x-ray to ensure the shoulder is back in joint and there are no associated fractures/broken bones. It is also advisable to immobilise the shoulder in a sling for a number of weeks for comfort. Often sedation or anaesthesia is required to reduce a dislocation and pain relieving medications are required for the next few days. We would recommend a medical assessment, including an x-ray of the shoulder, be required in all cases. Associated injury to bone, the cartilage of the shoulder (labrum), the lining of the shoulder (capsule) or surrounding muscles (rotator cuff) and nerves may complicate the injury and require further investigations. As a result; we would also recommend an MRI/Arthrogram after an instability episode, to assess the damage to the joint. This finer detail cannot be easily seen on x-rays.
If the shoulder pops out but pops back in without medical intervention it is called a subluxation (partial dislocation). This is still considered a type of shoulder instability.
In some players the shoulder doesn’t dislocate or subluxate but the player has pain with impact particularly when the arm is extended. This may be accompanied by loss of power, numbness or tingling . This is sometimes called a stinger.
What investigations are required?
The best scan for shoulder instability is an MRI scan where dye is injected into the shoulder (MR arthrogram). If there has been a recent dislocation, within the last 10 days, a plain scan with-out the dye, a non-contrast scan, may be sufficient. Our team can help in arranging the appropriate scans.
Shoulder Injuries
Treatment options available
Surgery is often required to treat shoulder instability. The surgery depends on the extent of the damage and future physical demands on the shoulder. However, if the patient is active and there is significant damage to the structures of the shoulder, a surgical reconstruction is recommended. This may be done either arthroscopically (minimally invasive surgery/ “keyhole”) or through an open incision. In those less-active patients who have little structural damage to the shoulder, physical therapy can help stabilise the shoulder without resorting to surgery in many cases.
It should be noted that with every subsequent dislocation further damage can be done to the shoulder joint and this predisposes you to osteoarthritis in the future.
The factors that influence whether surgery is recommended depend on the age of the patient, sports played, position in sports, number of either subluxations or dislocations, examination and findings on MRI scan. Despite advances in rehabilitation, strengthening and physiotherapy, the recurrence rate for shoulder instability is high (over 90% recurrence in 20-year-old males). That recurrence rate is far higher in those persons with bony and cartilage damage than those without.
Generally, in the young athletic population surgery is recommended as there is a high rate of further dislocations. If the patient has further dislocations more damage can be caused require a more extensive surgery. In the younger Athlete we may try and defer surgery until the patient is a little older and the body is more mature as surgery is more successful in the later teenage years and beyond. However even in the younger athlete, surgery may be preferable to multiple dislocations.
What Type of Surgery is preferred?
Arthroscopic Stabilisation (Keyhole procedure)
Arthroscopic stabilisation is a minimally invasive surgical procedure where the unstable shoulder joint is repaired through small “keyhole” incisions. The surgery is performed under general anaesthetic. Initially when asleep, your shoulder will be examined under anaesthetic, this allows us to assess the natural bony stability and laxity when the actions of muscle spasms are removed by the anaesthetic. Then, through a small 3mmm incision, a small camera will be inserted into the shoulder joint to confirm the amount of damage (labral tear) that was seen on your scans but also this allows us to check for any other, unseen or new damage, not on the scans to the bones and ligaments. A salt water fluid called saline is passed into the shoulder to allow us to better see the structures within it.
The area of bone where are the labrum has become detached is freshened and the anchors are inserted through additional small incisions. The anchors are made of a bioabsorbable (dissolvable) material, which is absorbed by the body after several months when the labrum has healed. Sutures (which are attached to the anchors) are passed around the torn labrum. When the sutures are tightened the labrum is firmly attached to the prepared bone allowing healing to take place. ( see figure x ).
The surgery can be accomplished using a number of these small, 3 mm incisions which generally heal well and are cosmetically pleasing.
Occasionally, if the degree of damage found at the time of the arthroscopy is greater than was demonstrated on the MRI scan or if the tissue quality is poor it may be necessary to convert to an open procedure which generally can be performed under the same general anaesthetic.
After surgery the wounds are covered with waterproof dressing so you can shower. You can use the arm below the elbow normally and generally use the shoulder enough to allow you to brush your teeth, use mobile phone and computer. The simple sling is easily removed for dressing. The sling is generally worn for three weeks. Patients who work in sedentary roles i.e. office based can generally return to work after one week.
Latarjet Procedure
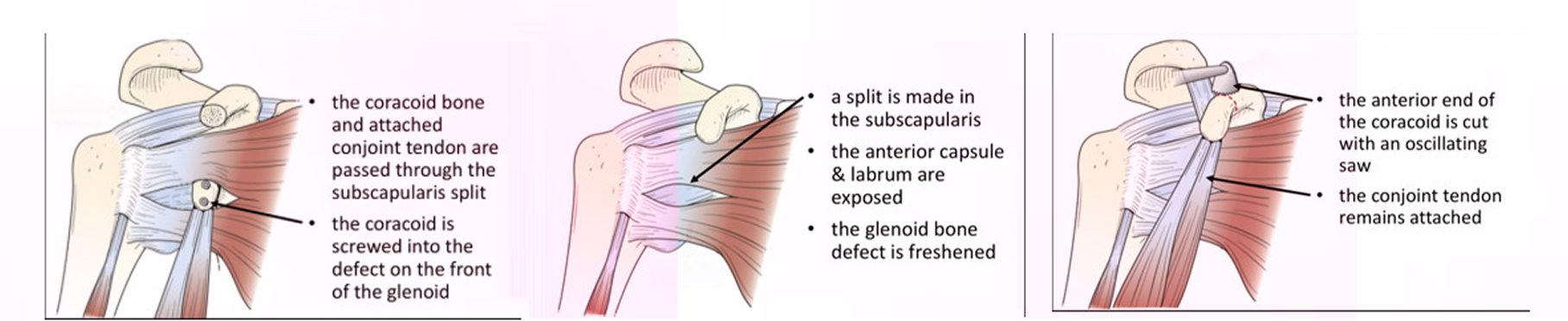
Latarjet Guide Latarjet Procedure – Open Shoulder Stabilisation Surgery
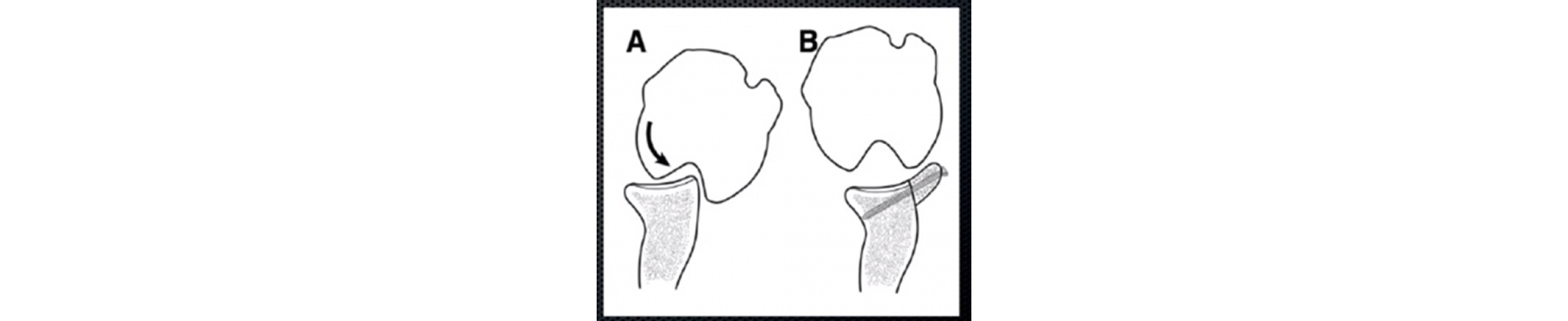
The Latarjet procedure is an operation to treat patients who have shoulder instability. It is often used in patients who play collision sports ,typically GAA or Rugby , who have sustained damage to the shoulder socket (glenoid) or the ball (humeral head) and have a high rate of dislocation .It has been used for many years and has the lowest failure rate of instability procedures particularly in patients who have sustained bone damage.
The surgery Itself:
The operation generally involves a single night in hospital and is performed under general anaesthetic. Your shoulder is always examined at the start of the case while the you are under anaethetic to assess the true instability while the muscles are all relaxed from the anaesthetic. Then a small 3mm incision is made at the back of the shoulder and the shoulder is inspected with a small camera (arthroscopy) to confirm the amount of bone damage seen on the scans and check for other potential injuries to the shoulder joint. A larger second incision is made over the front of the shoulder (approximately 6cm in length). The shoulder joint is exposed and the bony fragment from the socket is removed. The corocoid bone is carefully cut, prepared and shaped and attached to the shoulder joint socket using two metal screws. These are made of a titanium alloy, are biologically inert and do not need to be removed. The wound is closed with dissolvable sutures and covered with a waterproof dressing which allows showering. You can use their arm immediately for activities such as using phone and laptop, washing teeth and personal hygiene. A physiotherapist will give you, the patient, some simple exercises before you leave the hospital.
Post-Operative Rehabilitation
A simple sling is worn for a 3-week period. We can advise about return to driving which is generally at three weeks. The patient may use the whole arm, including shoulder, for light activity. Eight weeks– The patient may begin unrestricted, active use of the arm and shoulder. Three months – Most patients are reasonably comfortable, have a range-of-motion about half of what is normal, and experience some weakness. Six months – Most patients are pain-free (although they may experience pain during certain weather conditions), and have motion and strength which is returning to that of a normal level. *
Complications
The surgery is successful in approximately 95% of patients. The surgery is performed under general anaesthetic, which brings its own set of comlications. Specific to the latarjet; here is a small risk (<1%) of damage to nerves or blood vessels , infection or bleeding (haematoma)- which rarely needs a further operation. A small proportion of patients (<5%) develop recurrent instability following the procedure. Some patients have persistent discomfort which generally improves with time.
Post-operative follow-up
The first post-operative visit is generally around 2-3 weeks. We will check the wound and discuss the procedure and give a physiotherapy referral and a post opartive rehabilitation protocol. At four months a final review with x-ray is scheduled. Our team, in conjunction with the treating physiotherapist will be able to advise on return to training, contact and play.
Shoulder Injuries
Shoulder Injuries
Shoulder Injuries
Shoulder Injuries

")